Précis
In this retrospective study, investigators evaluated a pharmacy-led initiative in the emergency department (ED), finding a potential reduction in ED revisits and hospital readmissions, though results were not statistically significant.
Objective
This study aimed to describe and evaluate a pharmacy-led clinical initiative during an ED visit.
Study Design
This study is a retrospective cohort study.
Methods
Patients 18 years or older with a history of heart failure, myocardial infarction, stroke, atrial fibrillation, or chronic obstructive pulmonary disease were included. The initiative was at a community hospital ED, where the emergency medicine pharmacist provided enhanced medication education at admission using a teach-back method. Data were collected for 3 months before (usual care) and during the intervention (enhanced care). The primary outcomes were all-cause 30-day ED revisit and hospital readmission rates. Secondary outcomes included the incidence of patients readmitted with the same illness and the cost savings. The primary outcomes were compared between the groups using χ2 tests (statistical significance set at P <.05).
Results
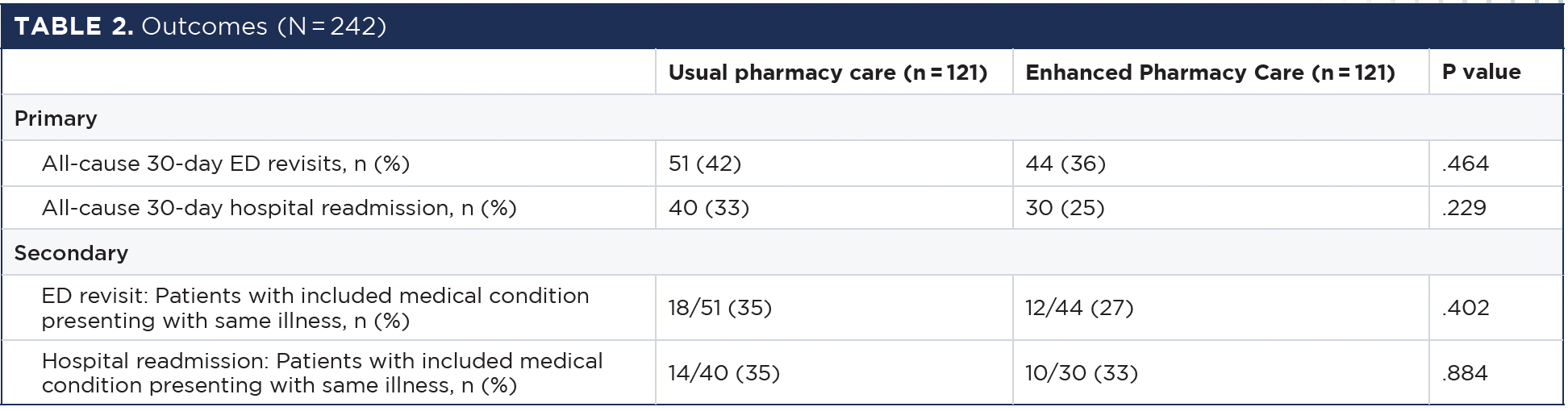
A total of 242 patients were included (121 usual vs 121 enhanced). There was a numerical decrease in all-cause 30-day ED revisits (usual 42% vs enhanced 36%, P = .464) and hospital readmission (usual 33% vs enhanced 25%, P = .229). Similarly, there was a numerical decrease in ED revisits (usual 35% vs enhanced 27%, P = .402) and hospital readmissions (usual 35% vs enhanced 33%, P = .884) due to the same illness. The pharmacy-led clinical initiative resulted in an estimated cost savings for the health system of approximately $177,506.
Conclusion
Although the pharmacy-led clinical initiative indicated a potential reduction in ED revisits and hospital readmissions, these findings were not statistically significant. Larger studies are needed to determine the intervention’s true impact on patient outcomes.
Introduction
Hospital readmission rates for chronic conditions are approximately 17%, with unplanned readmissions costing from $15 billion to $20 billion annually.1-3 The Agency for Healthcare Research and Quality reports that the 5 leading all-cause 30-day adult hospital readmissions are sepsis, heart failure, diabetes with complication, chronic obstructive pulmonary disease (COPD) exacerbation, and acute/unspecified renal failure.4 Patients experiencing these conditions often take multiple medications, which can complicate their understanding of what each medication is for, how it works, and the importance of adhering to their prescribed regimen. This lack of understanding may result in ED visits and hospital readmissions.
Pharmacists are essential in the medication management process, as they take medication histories and perform medication reconciliations, allowing them to identify and address medication-related concerns effectively. They provide valuable guidance on managing polypharmacy, adverse effects (AEs), and drug interactions while also educating patients about their medications to improve their understanding and adherence. These efforts have been shown to help reduce readmission rates.5,6
In a systematic review and meta-analysis of randomized trials, Kelly et al investigated the associations among pharmacist counseling, medication adherence, 30-day hospital readmission, and mortality, finding evidence supporting pharmacist counseling as a means to enhance medication adherence and decrease hospital readmissions and ED visits.7 Also, Clark et al evaluated the impact of a pharmacist-led hospital discharge medication reconciliation process and found that it was associated with a significant reduction in medication discrepancies on the discharge medication list and the adjusted odds of 30-day hospital readmission.8 Although previous studies demonstrated that medication education performed during the discharge process had positive outcomes, including decreased ED revisits and hospital readmissions, limited studies are available to show the impact of patient education at admission.9-12
The impact of patient education at the point of admission remains underexplored, with most studies focusing on discharge procedures. Our study addressed this gap by implementing a pharmacy-led clinical initiative during the admission process in the ED. This initiative was designed to improve patients’ and their caregivers’ understanding of their medications at an early stage, with the goal of enhancing medication adherence and potentially reducing hospital readmissions. The primary objective of our study was to evaluate the impact of this pharmacy-led initiative by comparing all-cause 30-day ED revisits and hospital readmissions between patients who received the intervention and those who did not.
Methods
Study Design and Setting
A pharmacy-led clinical initiative was implemented in the ED of a 260-bed community hospital from April to June 2022. The hospital has 2 full-time clinical pharmacy specialists and 2 full-time medication history pharmacy technicians who provide ED coverage and patient care. For this study, just 1 clinical pharmacy specialist and 1 medication history pharmacy technician participated, as they shared the same work schedule of four 10-hour shifts per week. The initiative focused on enhancing medication history and patient education during ED visits and was conducted exclusively during this period.
This study represents the initial implementation of a pharmacy-led clinical initiative in our institution’s ED. The focus was to assess the feasibility and potential impact of this intervention on patient outcomes. This work served as an initial evaluation of the program’s effectiveness and operational integration.
A retrospective chart review was conducted to evaluate the impact of this intervention. This review compared patient outcomes from the 3 months before the intervention (January through March 2022, referred to as usual pharmacy care) to those during the intervention period (April to June 2022, referred to as enhanced pharmacy care). The usual care cohort consisted of patients who received standard pharmacy care, whereas the intervention cohort included patients who received the enhanced pharmacy-led education and medication reconciliation services. The goal was to assess changes in ED revisits and hospital readmissions between the 2 cohorts.
Participants and Cohort Selection
Patients 18 years or older who were admitted to the hospital with a history of congestive heart failure (CHF), myocardial infarction, stroke, atrial fibrillation, or COPD were included in the study. The control cohort (usual pharmacy care) consisted of patients admitted during the preintervention period, whereas the intervention cohort (enhanced pharmacy care) included those admitted during the intervention period.
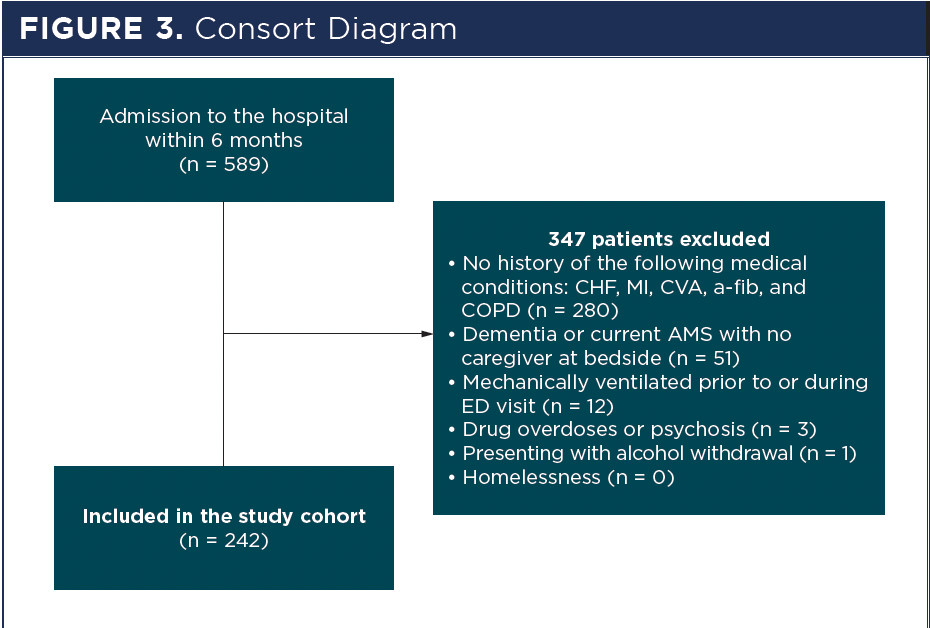
Patients were included if they were on at-home medications for any of the aforementioned conditions and had a complete medication history documented in the hospital’s system. Exclusion criteria included patients who were homeless, presented with alcohol withdrawal, drug overdoses, psychosis, dementia, current altered mental status without a caregiver present, or required mechanical ventilation before or during their ED visit.
No formal matching process was used; however, baseline demographics and clinical characteristics of the 2 cohorts were compared to ensure similarity. Patients in both groups were identified through a retrospective chart review using the hospital’s electronic medical record (EMR) system.
The medication history pharmacy technician performed screening for study enrollment, assessing each patient’s home medications using the ED-specific dashboard. The emergency medicine (EM) clinical pharmacy specialist then confirmed eligibility through chart reviews and consultations with EM physicians. Screening and patient education were conducted during the technician’s and pharmacist’s regular working hours.
Intervention
The enhanced pharmacy care intervention consisted of a detailed medication history assessment followed by an educational session conducted by an EM clinical pharmacy specialist. Figure 1 describes the intervention workflow. Initially, a trained pharmacy technician, serving as a medication history technician, collected detailed information on the patient’s at-home medications. This included documenting all prescribed and OTC drugs, herbal supplements, and adherence patterns. The technician also identified and documented any medication-related issues, such as discrepancies between the patient-reported medication list and the medical records, potential drug interactions, medication duplications, patient nonadherence, and any reported AEs. These issues were then communicated to the clinical pharmacy specialist for further evaluation and intervention. The technician used a standardized medication history assessment form to interview patients and/or caregivers (Figure 2).
After medication history was collected, patients included in the enhanced pharmacy care received educational medication intervention from the EM clinical pharmacy specialist. These in-person educational sessions focused on disease states, medication indications, administration, and monitoring instructions. To assess their understanding and to reiterate medication adherence, patients and/or caregivers are requested to perform a teach-back to the EM clinical pharmacy specialist detailing the information discussed. For individuals who could not speak or understand English or were deaf, an interpretation service provided by the institution was used. A summary of the patient’s interaction and education session was documented in the pharmacy record. All educational tools for the enhanced group were created by the EM clinical pharmacy specialist with internal department review. This study was meant to test and evaluate the feasibility and effectiveness of the tool.
Outcomes Measurement
Patients were followed up to 6 months post intervention for outcome measurement. The primary outcomes measured were all-cause 30-day ED revisit and hospital readmission rates. ED revisits were defined as any return to the hospital’s ED within 30 days of the index visit. Hospital readmission was defined as any inpatient stay within 30 days after discharge from the index hospitalization.
It is important to note that these outcomes were limited to data captured within our hospital’s EMR system. As a result, the analysis just included revisits and readmissions that occurred within the same health care system. This may not fully capture all patient encounters, especially if patients sought care at another facility outside our health system. This limitation meant that the results are not directly comparable to Centers for Medicare & Medicaid Services readmissions rates, which include data from multiple health care facilities and are used for value-based payments. The cost-savings calculations were derived using average cost estimates from the hospital’s finance department and were adjusted for diagnosis-related group, types of services rendered, volume, and the month of the visit. Readmission penalties varied depending on the payer. Our hospital received reimbursement for some readmissions, so the cost of readmission just applied if we were not reimbursed. In such cases, the hospital absorbed the financial burden and revenue loss.
Statistical Analysis
Descriptive statistics were used to summarize patient demographics and baseline characteristics. For the primary analysis, inferential statistics were employed to compare the outcomes between the usual care and enhanced pharmacy care cohorts. χ2 tests were used for categorical variables, such as rates of ED revisits and hospital readmissions, whereas t tests or Mann-Whitney U tests were used for continuous variables, depending on data distribution. Statistical significance was defined as a P value of less than .05 for all analyses. Data were analyzed using the statistical software Minitab version 18.
No formal sample size was conducted before the study, as the study was limited by the availability of resources, specifically the manpower of the pharmacy team, which included just 1 full-time clinical pharmacist and 1 medication history technician. These personnel constraints, combined with the demands of clinical responsibilities, restricted the number of patients who could be included in the study.
As this study was a performance improvement project focusing on educational interventions, it was granted an exemption from review by the Memorial Hermann institutional review board.
Results
Participant Characteristics and Enrollment
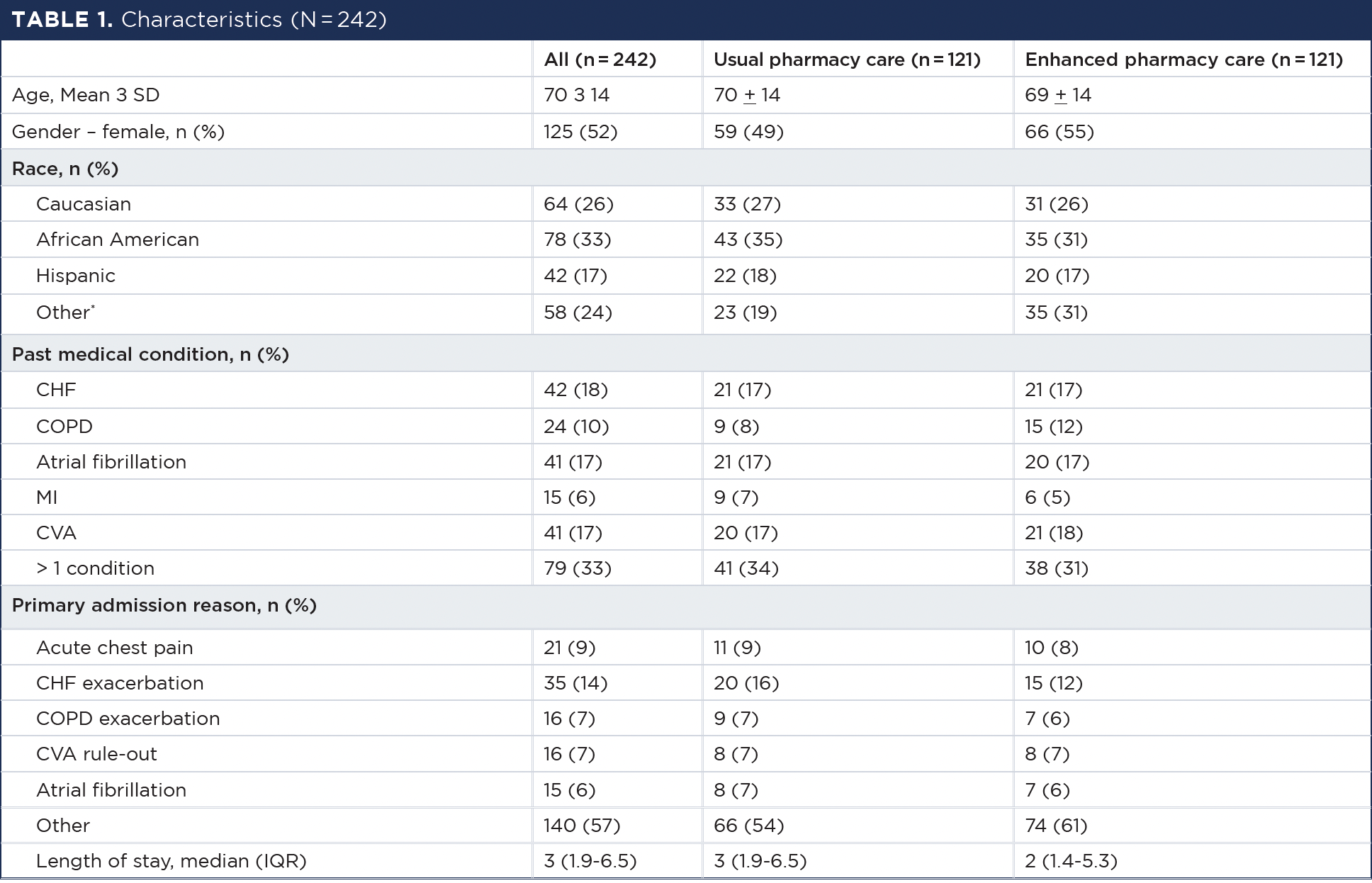
Of 589 patients admitted to the hospital, 242 patients (41%) (121 usual vs 121 enhanced) were included in the study (Figure 3). Fifty-two percent of patients were female, 33% were African American, and 26% were Caucasian, with a mean age of 70 years (SD, 14) (Table 1). Of the included patients, 31% of admitted patients had more than 1 medical history, with CHF being one of the most common medical history conditions. Baseline demographics and clinical characteristics were similar between groups (Table 1).
Nonadherence was categorized into 2 types: intentional and unintentional. Intentional nonadherence occurs when a patient chooses not to follow treatment recommendations based on their beliefs and preferences. In contrast, unintentional nonadherence happens when a patient intends to follow the recommendations but encounters practical obstacles, such as poor recall or forgetting to take medication regularly. During the education session, the primary reason for at-home medication nonadherence was a lack of understanding (n = 73; 60%), followed by polypharmacy (n = 36; 30%). While there is no standard definition of polypharmacy, the term is commonly defined in the literature as the regular use of at least 5 medications. Consequently, we have adopted this definition for our purposes as well. The most common area of education provided to patients was medication indication (n = 54; 45%), followed by compliance (n = 42; 35%), and lastly monitoring (n = 24; 20%). The estimated median time spent on each patient was 25 minutes (range, 18-35 minutes).
Outcomes
There were numerical decreases in all-cause 30-day ED revisits (usual 42% vs enhanced 36%, P = .464) and all-cause 30-day hospital readmissions (usual 33% vs enhanced 25%, P = .229). Both reductions were not statistically significant.
There were numerical decreases in ED revisits (usual 35% vs enhanced 27%, P = .402) and hospital readmissions (usual 35% vs enhanced 33%, P = .884) due to the same illness (Table 2).
The pharmacy-led patient education program was associated with an estimated cost savings of $177,506 for the health care system, based on the reduction in ED revisits and hospital readmissions. The estimated cost-saving was specific to this hospital and may not be generalizable to other settings due to variations in health care costs and resource use.
Discussion
Our study observed numerical reductions in all-cause 30-day ED revisits and hospital readmissions among patients who received enhanced pharmacy care during their admission (6% and 8% reductions, respectively). However, these differences were not statistically significant, indicating that we cannot be certain these reductions reflect the true effects of the intervention.
Our findings were consistent with previous research suggesting that pharmacist involvement can improve medication adherence and reduce health care use. However, this study alone does not provide sufficient evidence to claim the pivotal role of pharmacists in this setting. The clinical significance of these interventions remains to be determined through larger, adequately powered studies that can more accurately evaluate both their statistical and practical implications. Previous studies have demonstrated that education performed during the discharge process had positive outcomes, such as a decrease in ED revisits and hospital readmissions; however, limited studies are available to show the impact of outcomes on the admission side.13-15 Zemaitis et al conducted a prospective, controlled study evaluating the impact of a pharmacy-facilitated medication reconciliation and patient education model with postdischarge follow-up on 30-day readmissions. The findings resulted in a 27% reduction in readmission during the intervention period.16 In another study, Bach et al performed a meta-analysis to evaluate the effectiveness of interventions involving pharmacists to reduce hospital readmissions, finding that 55% of studies showed a statistically significant reduction in readmissions ranging from 3.3% to 30%, with most of the interventions focused mainly on patient education.17
Clinical pharmacists have a unique opportunity to improve patient care through medication education activities at the entry point of hospital admission. Our focus was primarily on the admission side for various reasons, including the fact that family members or caregivers are often present during the admission period, making it easier to gather medication history and provide education on disease states and medications. As a result, there will be overall increased understanding and adherence.
Furthermore, increased patient and caregiver knowledge, in addition to a medication list provided by the EM clinical pharmacy specialist, will facilitate a more substantial discussion with the admitting clinical team from all involved parties. The teach-back method used in our enhanced care protocol proved effective in ensuring that patients understood their medication regimens and the associated management of their conditions. This method has been endorsed in other studies to enhance patient understanding and adherence, which are critical for preventing readmissions.18-20 However, implementing such interventions in the high-pressure environment of the ED presented unique challenges, including time constraints and the need for pharmacists to balance multiple responsibilities. Despite these challenges, our study highlighted the potential for significant cost savings and improved patient care, supporting the argument for pharmacists’ roles to be focused on care transitions. Optimally, patient education should consist of a coordinated series of efforts.
Study Limitations
This retrospective analysis did have several limitations. The effects were not necessarily generalizable to a broader population and setting because it was conducted at a 41-bed ED with a small sample size. The study’s small sample size significantly affected the statistical power of the analysis.
A post hoc power analysis was conducted to assess the study’s ability to detect differences in the primary outcome of all-cause 30-day ED revisits. Based on the observed effect size and assuming an 80% power and a 95% confidence level, the study would have required approximately 1037 participants per group to achieve adequate power. Given that just 121 patients were included in each group, the study was underpowered, limiting its ability to determine the true effectiveness of the pharmacy-led intervention.
Other limiting factors included a shortened intervention time and nonmatching groups; additionally, our EMR does not capture ED revisits and hospital readmissions information if patients went outside of our health system. Additional education and the review of medication use to minimize AEs, among others, may have been introduced during hospitalization and could have potentially impacted the results.
About the Authors
Vy P. Pham, PharmD, BCPS, is an emergency medicine clinical pharmacy specialist in the Department of Pharmacy at Memorial Hermann Greater Heights Hospital in Houston, Texas.
Marisol Ramirez, CPhT, is a medication history pharmacy technician in the Department of Pharmacy at Memorial Hermann Greater Heights Hospital in Houston, Texas.
Amit Patel, MD, is an emergency medicine physician in the Department of Emergency Medicine at Memorial Hermann Greater Heights Hospital in Houston, Texas.
Lan N. Bui, PharmD, MPH, CPS, is an associate professor of pharmacy practice in the Department of Pharmacy Practice at Lloyd L. Gregory School of Pharmacy in West Palm Beach, Florida.
Due to the nonsignificant nature of the results, we acknowledge a potential limitation in statistical power, as no formal power calculation was conducted before the study. This limitation may have affected our ability to detect smaller but clinically meaningful differences between the groups.
As pharmacy involvement in medication history and reconciliation grows, additional research will be necessary to reproduce these findings through comparable educational interventions performed during both the admission and discharge sides. Furthermore, future studies can explore whether this educational intervention leads to improvements in in-hospital outcomes, such as reduced length of stay, appropriate medication use, fewer AEs, and enhanced adherence.
Conclusion
Within the 3-month study period, the pharmacy-led clinical initiative was associated with numerical reductions in ED revisits and hospital readmissions. However, these reductions were not statistically significant, and the study was underpowered to detect meaningful differences due to its small sample size. Although the results suggest a potential benefit of pharmacist-led interventions, further research with larger sample sizes and robust study designs is needed to conclusively determine the effectiveness of these educational initiatives.
REFERENCES
Brunner-Rocca HP, Peden CJ, Soong J, Holman PA, Bogdanovskaya M, Barclay L. Reasons for readmission after hospital discharge in patients with chronic diseases—information from an international dataset. PLoS One. 2020;15(6):e0233457. doi:10.1371/journal.pone.0233457
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428. doi:10.1056/NEJMsa0803563
Medicare & Medicaid Statistical Supplement. Centers for Medicare & Medicaid Services. 2007. Accessed March 30, 2024. www.cms.hhs.gov/MedicareMedicaidStatSupp/downloads/2007Table5.1b.pdf
Weiss AJ, Jiang HJ. Overview of Clinical Conditions With Frequent and Costly Hospital Readmissions by Payer, 2018. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US); July 20, 2021.
Gallagher D, Greenland M, Lindquist D, et al. Inpatient pharmacists using a readmission risk model in supporting discharge medication reconciliation to reduce unplanned hospital readmissions: a quality improvement intervention. BMJ Open Qual. 2022;11(1):e001560. doi:10.1136/bmjoq-2021-001560
Lázaro Cebas A, Caro Teller JM, García Muñoz C, et al. Intervention by a clinical pharmacist carried out at discharge of elderly patients admitted to the internal medicine department: influence on readmissions and costs. BMC Health Serv Res. 2022;22(1):167. doi:10.1186/s12913-022-07582-6
Kelly WN, Ho M, Bullers K, Klocksieben F, Kumar A. Association of pharmacist counseling with adherence, 30-day readmission, and mortality: a systematic review and meta-analysis of randomized trials. J Am Pharm Assoc (2003). 2021;61(3):340-350.e5. doi:10.1016/j.japh.2021.01.028
Clark CM, Carden D, Seyse S, Cieri-Hutcherson NE, Woodruff AE. Impact of pharmacist-led discharge medication reconciliation at an academic medical center. J Am Coll Clin Pharm. 2023;6(5):458-465.
Patient-Centered Care. Robert Wood Johnson Foundation. Accessed February 6, 2025. https://www.rwjf.org/en/insights/collections/patient-centered-care.html
Chisholm-Burns MA, Kim Lee J, Spivey CA, et al. US pharmacists’ effect as team members on patient care: systematic review and meta-analyses. Med Care. 2010;48(10):923-933. doi:10.1097/mlr.0b013e3181e57962
Lada P, Delgado G Jr. Documentation of pharmacists’ interventions in an emergency department and associated cost avoidance. Am J Health Syst Pharm. 2007;64(1):63-68. doi:10.2146/ajhp050213
Bonetti AF, Reis WC, Mendes AM, et al. Impact of pharmacist-led discharge counseling on hospital readmission and emergency department visits: a systematic review and meta-analysis. J Hosp Med. 2019;15(1):52-59. doi:10.12788/jhm.3182
Lázaro Cebas A, Caro Teller JM, García Muñoz C, et al. Intervention by a clinical pharmacist carried out at discharge of elderly patients admitted to the internal medicine department: influence on readmissions and costs. BMC Health Serv Res. 2022;22(1):167. doi:10.1186/s12913-022-07582-6
Tasseff N, Axtell S, Nixon B. Effect of extended pharmacist involvement in discharge transitions of care on hospital readmission rates: prospective, randomized, parallel arm design trial. J Am Coll Clin Pharm. 2024;7:8-14.
Peasah SK, Hammond T, Campbell V, et al. Assessing the impact of adding pharmacist management services to an existing discharge planning program on 30-day readmissions. J Am Pharm Assoc (2003). 2022;62(3):734-739. doi:10.1016/j.japh.2021.12.005
Zemaitis CT, Morris G, Cabie M, Abdelghany O, Lee L. Reducing readmission at an academic medical center: results of a pharmacy-facilitated discharge counseling and medication reconciliation program. Hosp Pharm. 2016;51(6):468-473. doi:10.1310/hpj5106-468
Bach QN, Peasah SK, Barber E. Review of the role of the pharmacist in reducing hospital readmissions. J Pharm Pract. 2019;32(6):617-624. doi:10.1177/0897190018765500
Yen PH, Leasure AR. Use and effectiveness of the teach-back method in patient education and health outcomes. Fed Pract. 2019;36(6):284-289.
O’Mahony E, Kenny J, Hayde J, Dalton K. Development and evaluation of pharmacist-provided teach-back medication counselling at hospital discharge. Int J Clin Pharm. 2023;45(3):698-711. doi:10.1007/s11096-023-01558-0
Cabilan CJ, Boyde M, Currey E. The effectiveness of pharmacist-led discharge medication counselling in the emergency department (ExPLAIN): a pilot quasi-experimental study. Patient Educ Couns. 2019;102(6):1157-1163. doi:10.1016/j.pec.2019.01.020
Acknowledgement: The investigators would like to thank the Department of Pharmacy and the Emergency Department at Memorial Hermann Greater Heights Hospital for providing administrative, intellectual, and information technology support. The investigators would also like to thank the Finance Department at Memorial Hermann Greater Heights/Memorial City Hospitals for providing cost data and assistance.













 -- CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CVA, cerebral vascular accident; IQR, interquartile range; MI, myocardial infarction. There was no significant difference between 2 groups across all variables. Other: Pacific Islander, Middle Eastern, and American Indian.")

 -- ED, emergency department.")